This week marked my 11th week in treatment for my mallet finger. Almost three months caring for this injury. 9 weeks in a cast. About 9 days in a splint 24/7. One week in a splint most of the day, taking it off 5X a day for an hour.
This morning was my third had rehab appointment since the cast came off. They also did the casting so I had two previous visits with them.
Typically, I go in, they make me bend my fingers and they measure everything, tell me the following week’s directions and send me on my way.
Today I went in, the had me heat my hand for 15 minutes and then I got a finger massage. The therapist measured my finger and made me a new night-time splint and told me I no longer need to wear the splint during the day.
Because I do so much work with my hands, if it starts to droop or just bothers me, I can splint it here and there for an hour.
I have another appointment with my hand surgeon July 27, so although the general guidelines say I only have to splint at night for 2 more weeks, it is recommended that I wear it until I see my specialist.
Other wisdom from my therapist as we chatted today:
Completely immobilizing a mallet finger for six weeks is the minimum in his opinion.
The finger can continue healing for an additional six months after splinting is complete. He recommends using individual judgment and awareness of the finger to decide how long to splint at night.
Massage the finger, especially the joints for five minutes several times a day.
Understand that the finger may never resume its former shape/posture/movement but that the end of the finger itself doesn’t have that big of a role in hand function.
Keep bending the fingers several times a day, gradually working into a fist.
I had an 8 a.m. appointment with my occupational therapist at The Institute for Hand and Upper Extremity Rehabilitation. I cannot say enough nice things about them.
I arrived around 7:50 a.m., and ended up walking into the building with my therapist. The receptionist wasn’t there yet. My therapist grabbed my file and started my appointment before her computer fully engaged for the day.
I told her the story of losing my splint. She made me a new one and I didn’t even have to pay extra.
The finger is “holding up” and this week, when I take the splint off to do my exercises five times a day— which I might do seven, just based on my routine— I can leave the splint off for one hour five times a day.
It sounds like if my finger maintains its posture through this week that I am more-or-less out of the woods. It’s very exciting.
Why do I do my exercises seven times a day? For exercises like these— physical and/or occupational therapy exercises that require little bits of effort multiple times a day— I find attaching them to logical parts of my routine helps.
So in my case:
I left my appointment at 8 a.m. They are so efficient!
4:15 a.m. Wake. Remove splint. Use bathroom. Wash hands. Start coffee. Do exercises. Replace splint.
6:15 a.m. Use bathroom at work. Check hair. Remove splint to wash hands. Return to main cafeteria to chat with friends. Do exercises as warm-up for the intense folding of clothes to come. Retape splint. Head to time clock.
8:50 a.m. Remove splint. Go to bathroom and take morning break. Do exercises. Have morning yogurt. Replace splint. Fold more clothes (about 175 pieces of clothing every two hours). Yes, I fold and package clothes. I work for Stitch Fix doing Quality Control for the subscription boxes. My side hustle is my book company, Parisian Phoenix Publishing.
12:10 p.m. clock out for lunch. Remove splint. Use the restroom. wash hands. Do exercises while heating lunch. Eat. Replace splint.
3:10 p.m. Final 15. Remove splint at work station. Go to wash hands. Do exercises while enjoying a cup of coffee or snack in the main cafeteria.
5 p.m. Clock out of work, remove splint, wash hands, stretch fingers, replace splint.
5:30 p.m. Get home from work. Fight off very excited large dog. Remove splint. Wash hands. Do exercises. Replace splint.
7:30 p.m. Remove splint. Shower. Gently use fingers to wash hair. Do exercises in shower. Dry off. Replace splint with fresh tape.
And this way if I miss one, it’s okay. Or if my hand isn’t doing as much in one session we make it up in the next.
So, as directed by my doctor, I went to see my friends — the occupational therapists at the Institute for Hand and Upper Extremity Rehabilitation.
They fitted me with a custom splint molded to my finger (for $50) that despite my doctor’s recommendation that I wear the splint at night only, they want me to wear the splint 24-hours a day for the next week, which for me will be nine days because that’s the day I can get there again.
I am to remove this splint when I bathe, when I wash my hands, and five times a day to do physical therapy exercises.
The exercises are 10 reps of basic hand gestures: straightening the hand, lightly bending the top of the hand, and making a loose fist.
If the hand loses progress instead of gains it, then the cast will be reapplied.
In pondering this, I realize several opinions of mine that may be greater truths:
Had I accepted my doctor’s solution of “cheaping out” and reusing my stinky cast as a splint, my recovery from this mallet finger would be more direct versus gradual. I believe gradual, supervised steps toward healing are better and I wonder if there are statistics about patients and the long-term success rates with these injuries with various treatments. How many patients would hear that insurance won’t cover it and end the conversation there without considering that the $50 might provide more than just a splint, but also guidance and expertise.
Are my occupational therapists just over-cautious or it is a case (as I think it is) that the therapists see more of this injury and in the same manner than nurses often know more than doctors, do occupational therapists understand more about function than fancy specialized surgeons?
I was very apprehensive and so excited to see my doctor at OAA today to get my damn cast off for an evaluation of my mallet finger.
The teenager texted me as I sat in the exam room.
“Free the finger!”
They had a devil of a time cutting it off— apparently after even five weeks in the same cast it was firmly on.
Both the hand/orthopedic specialist and the hand rehab office it’s unusual for patients to maintain a finger cast for so long. That doesn’t make sense to me, because why wouldn’t you do everything in your power to maintain agility and strength in yourfinger?
Free the Finger!
the Teenager
And don’t give me that “it’s too hard” or “I need my hand to do stuff.”
I work in the Stitch Fix Bizzy Hizzy warehouse folding clothes. And after my brief stint on short term disability to deal with my balance and hip issues stemming from cerebral palsy (and made more complicated by now not being able to rely on the left side of my body with this temporary injury), I went back to work and performed at 100% and higher with my finger in a cast and restricted hand movement.
That finger had so much caked dead skin and here’s the really fascinating part— my knuckle no longer has wrinkles because it has not bent.
In the beginning of my treatment, I found my doctor cold and impersonal but as he gets to know me I like him more and I get more personable interactions from him.
He told me I should gradually increase my finger flexibility with care not to hyperextend it (otherwise known as don’t bend it backwards) and splint it at night. For the splint, I could take my cast back. And tape it in at night.
“It’s cheap, but it’s dirty,” the doctor said.
Yeah, no thanks. I lived with that grimy thing long enough.
“The other option is to return to the Hand Institute and they’ll make you a splint.”
(Which, coincidentally Cigna, my insurance, does not cover. But as I do not cheap out on my medical care, I will pay for. Because right now my HSA is empty because having a disability and doing everything you can to keep yourself ahead of that disability is expensive. So please, consider this and how lucky I am that I can support myself because if I had to really on family and government benefits to subsidize my care, I’d be crippled.)
I imagine there’s a third option— buy an over-the-counter splint. And I was going to consider that. But to me, the cost of the custom splint comes with the knowledge and enthusiasm of the people at the Institute for Hand and Upper Extremity Rehabilitation. These people love and know hands.
And if I can only teach others one concept about your health, it is this: invest in yourself, meaning, find the right medical providers for your team that understand your needs and share your personal philosophy and concerns. This requires being vulnerable in a way that might be uncomfortable and it might mean having difficult conversations with people you don’t like. But it may also lead you to better understanding of yourself and of those people who seemed like callous know-it-alls disinterested in you.
I peppered my hand specialist with questions today— rapid fire as he typed my splint referral into the computer. And he respected them. The questions.
How much movement is okay? What should I watch for? I pack boxes and fold clothes and put things on conveyer belts. Should I splint the finger at work if it starts to feel weird? Is there certain motion I should avoid?
“There are no rules,” he said. “Just be careful and the occasional splinting wouldn’t be bad. I’ll see you in a month.
He made eye contact with me as if to say, “you know your body. Follow your gut.”
But he also knows I’m the patient who kept a finger cast on longer than the average Joe. So maybe, just maybe, he trusts me.
For previous installments on my finger injury: click here.
If you read my post from earlier today, then you already know my hand specialist/orthopedic surgeon cut off my cast.
No more man with hat.
This meant I had to schedule an appointment with the very amazing staff at The Institute for Hand and Upper Extremity Rehabilitation for a new cast.
This also meant I had to cancel my session with Andrew at Apex Training.
At the time I should have been sweating, the teenager and I were cruising down the highway.
The staff member who originally wrapped my finger anxiously stood by as a newer staff member removed the temporary splint.
“You look like you’re waiting for someone to open a present,” I said.
She was that excited to see how I was healing.
My finger is straight, which means the tendon is growing in the right direction. It does not have enough tissue to have any strength yet, so another cast was put on.
I was in and out in 15 minutes, including my trip to the bathroom.
FURR Louise
In other news, our remaining two foster who needed shots made it to the vet today. While I was rocking temporary splints.
My soul, although surrounded by so much goodness and spring happy vibes, trembles in stress most of every day.
2022 has challenged me.
And that’s okay.
Today I visited my hand specialist for my first monthly follow-up of my ruptured tendon in my left ring finger, an injury known as “mallet finger” or “baseball finger.”
Here are some of my previous posts about the injury:
My specialist removed my cast tonight and announced my performance at holding my finger up is halfway there.
Then he also announced I’d need a splint or a new cast.
I made the appointment for my follow up at the office close to home only to have him call me and tell me I need to see the hand institute by his office on the other side of the valley. 30 minute drive.
At the end of a very busy week that includes my birthday.
I have to take some foster cats to the vet at 1, and run over to my occupational therapist’s office for a 3:30 appointment. I called from the parking lot of the specialist.
Then I had to come home and crate 3 cats for their vet appointment so now my temporary splint is very fuzzy.
I’ll update later based on what the next phase of treatment is. Whatever it is, I hope we can wash my hands first.
Today I went to see my family doctor as I am concerned about the interaction of my mallet finger and my list of comorbidities from cerebral palsy. My crooked gait makes me a fall risk and the last five years or so— more or less since I entered my forties— have included broken bones, SI joint pain, back pain and hip pain.
All of this have led to a more-than-one-year journey to understand my body and how cerebral palsy impacts it.
I have visited doctors and specialists and neurologists trying to understand what I can do to minimize further issues as I age.
And it has worked!!!! My pain levels and chronic issues have dropped from daily pain of 5-8 to pain levels.
So I had a long visit with my primary care physician and told him not only about my injury, but also updated him on my fitness and improvements. I explained how I have been learning how muscles are supposed to work with my friends at Apex Training. I also told him I fell onto the brick wall of my house yesterday. I showed him the abrasions on my left arm.
Then I pointed out that traditionally my left side has been my anchor and by removing that from the anchor position, my walk has become more asymmetrical (according to my iPhone) and my hip is out of whack and uncomfortable all of the time and it’s only getting worse in these conditions.
Unlike the specialist— he filled out the paperwork himself and in front of me requesting that I have an FMLA leave until he sees me again after my specialist.
On top of all of that attention, he then gave me a full physical.
It was very hard for me to be vulnerable and ask for help, and my doctor and his staff made me feel heard, valued, and as if they truly cared about me.
I brought the paperwork home and started the claim process to initiate a short-term disability leave. It took about an hour and I realized my doctor missed one of the pages and on another he misread the questions. (So I added post-it notes.)
And if I’m 100% honest, despite everything I deal with, I still harbor feelings of guilt for asking for this time— much of which I intend to use doing work with my personal trainer and chiropractor to strengthen this hip and improve my walk so I can return to my warehouse job with a strong core and a better understanding of how normal legs work. I’m going to try to teach them. But, with my femoral anteversion, I know there is only so much I can do.
I deserve a chance to make myself strong and healthy.
It’s Tuesday and my life has been turned upside down by my “mallet finger” injury acquired Friday night, taking off my socks as I chronicled here.
I filed for short term disability leave based on what Patient First told me about the injury. Since my work week starts on Sunday, and the accident happened Friday night I thought it best to get the incident in the system as soon as possible.
The original injury left me with a finger that would not straightenAt Patient First
With it happening on Easter Weekend, I was told by the doctor at Patient First to make an appointment with an orthopedic hand specialist Monday.
The doctor at Patient First explained that I had pulled the tendon out of my knuckle and that I needed a specialist to determine whether it would heal or if I needed surgery.
And I did my best to work around my enormous splint and changed the tape once Sunday night.
Even on Sunday night, I had no pain, minimal swelling and no bruising or discoloration. The nail was fine, too. And I was amazed at how the angle of the finger had improved.
48 hours after injury The angle of my mallet finger 48 hours after original injury
Some recommendations came my way from friends and everyone recommended the same doctor at OAA Orthopedic Specialists. Unfortunately, he was booked into July. So I accepted an appointment with one of his colleagues, at an office 18 miles from my house. I called at Monday morning 8 a.m. and the only appointments they had this week were Tuesday at this office in the Allentown area.
That was today. The splint Patient First gave me is enormous— and I was very anxious to get not only news and a treatment plan, but also something more reasonable.
I filled out all the paperwork I could online, and headed out of the house for the 30-minute drive to the doctor. On Monday, I had already gathered my x-rays and reports from Patient First, a release of medical information form, my return-to-work form for the Stitch Fix Bizzy Hizzy and the FMLA/short-term disability insurance paperwork.
(I also tried to clean the Tupperware cupboard, loaded and unloaded the dishwasher and made an enormous homemade Crunchwrap with homemade tortilla chips.)
I cried all the way down the highway. I miss my dad, who passed away in December, and I’m struggling with a lot of life right now. And I snapped driving to the specialist.
But when I arrived— h*ly sh*t. The orthopedic office shared a plaza with the Lehigh Valley Hospital Cancer Center and the Steel Fitness Premier Facility. The scheduler told me they had free valet parking but damn I did not expect that. It was a big hospital facility.
I went in, read the directory and discovered my office was on the second floor. And when I got to the second floor, I saw about ten check-in/ receptionists. Damn.
One checked me in and I was told to proceed to waiting room seven. The whole arrangement vaguely reminded me of the Beetlejuice scene where the dead people wait to see their counselor.
But they moved me right along and I met my doctor very quickly. And I was told getting dressed and undressed is a common way of getting injured.
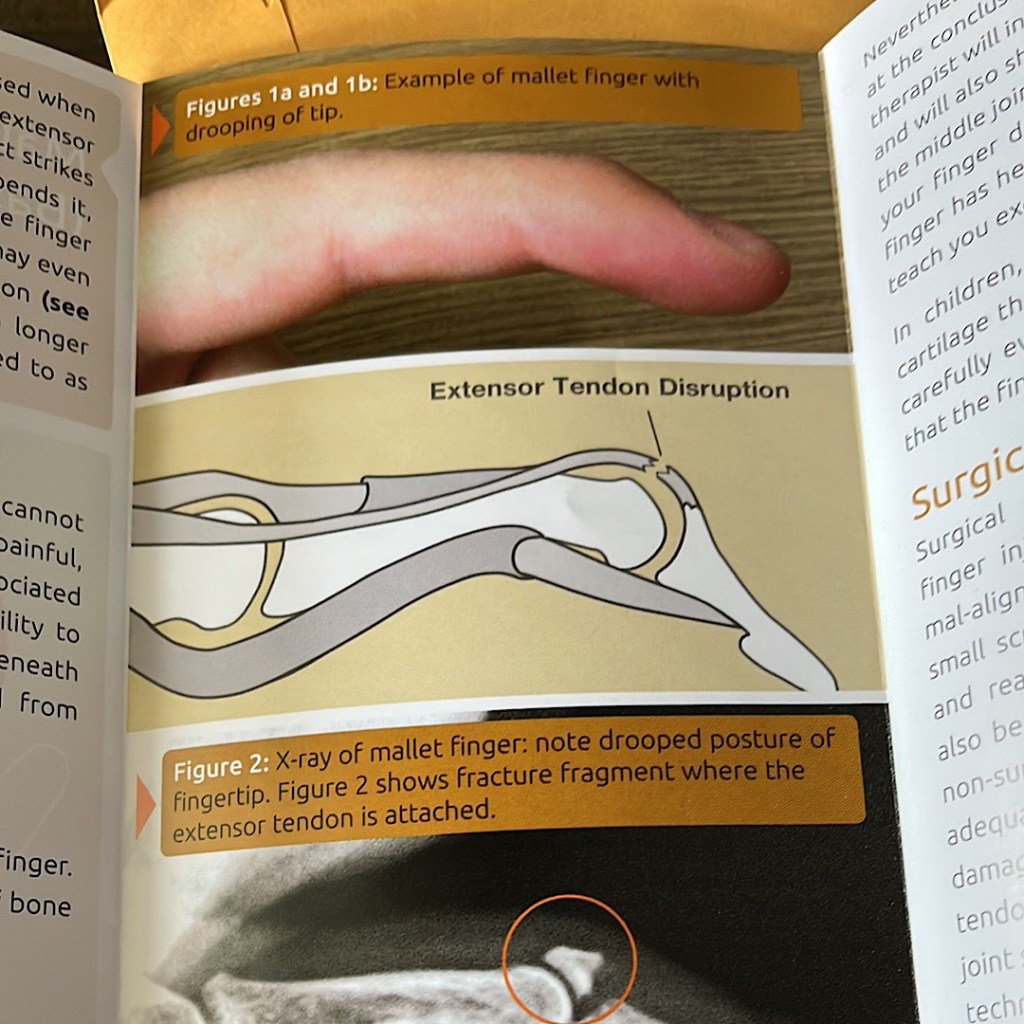
The doctor produced a brochure from a nearby drawer. And it was the same information from the same hand specialist professional organization I had found online.
He explains that there are two tendons in each finger, one running along the top from knuckles to fingernail, and another running under the finger. I overextended the top tendon at that tip-top knuckle, tearing it from the joint.
Because I did not damage or break free any bone, this means I don’t necessarily need surgery. That immobilizing the finger at the top knuckle will allow the scar tissue to reconnect the tendon. And then occupational therapy will get that tissue usable.
The mallet finger brochure
The doctor said there are three treatment options:
Splint
A surgically-placed pin
A finger cast
He recommended the finger cast. For eight weeks. And that he will see me in four weeks.
Paperwork and work release proved to be more complicated. He simply gave me a note asking me not to use the finger and that I could return to work today. I don’t think that’s enough for the folks at the Bizzy. So I asked the staff to please fill out the two forms— the one for the Bizzy Hizzy and the one for disability insurance— and told them I had read the sign and would gladly pay the $10 per form.
They wanted fax numbers or for me to pick up the forms, but I’m not driving 30 minutes back tomorrow or whenever they get the forms done. I think I found the fax for the disability folks and finally reneged and let them mail the form to my warehouse.
They also told me the forms should be in my portal so when they are done I hope I can download from the portal and send them where they need to go. If that doesn’t work, I have to call the Bethlehem office and make arrangements to pick them up there.
The OAA office also called The Institute for Hand and Upper Extremity Rehabilitation (a mere mile away) and arranged for them to see me. When I arrived, they were on the phone with my insurance company.
The staff at The Institute were beyond friendly, and every staff member apologized for making me wait. But I was impressed at how smoothly they ran and how they managed to balance the walk-ins and the scheduled patients.
Even more impressive, they had a binder promoting the small businesses they have “interacted” with— I hope I can leave one next time. I forgot by the end of my visit.
The Institute has one main rehab room so I got to see other patients at work, and every therapist acknowledged me, and apologized that I was waiting. One therapist, fitting a patient with some sort of brace or sling, was chatting with me about my injury.
The casting process was fascinating as I had never heard of casting a finger before and the person helping me also explained my injury. In this day and age when medical professionals usually don’t explain things, I was amazed at how many people took time to explain.
Mallet finger cast
My finger was only 15 degrees floppy today, which is a huge improvement from Friday. BUT if anything bends the injured area of the finger that could start the recovery clock back to zero as it could tear the scar tissue (which is why the hand specialist recommended the cast).
I certainly don’t relish the idea of eight weeks in a finger cast, nor do I enjoy the paperwork hurdles I now have to jump, but I’m relieved to have moved on to the next stage of the process.
The staff at the Institute also commended me for seeking treatment right away, as most people wait a week or more to address it and that causes more stress and damage to the healthy parts of the finger and can make the healing process more complicated and less successful.